
Update April 13, 2018: MAHC issued a subsequent media release regarding the latest update which you can read at the end of this post
The Capital Plan Development Task Force met on March 19 and 26 where the task force arrived at two important milestones. The task force approved the evaluation criteria to be used to evaluate the models, and finalized the different programs and services proposed in each of the models as described below.
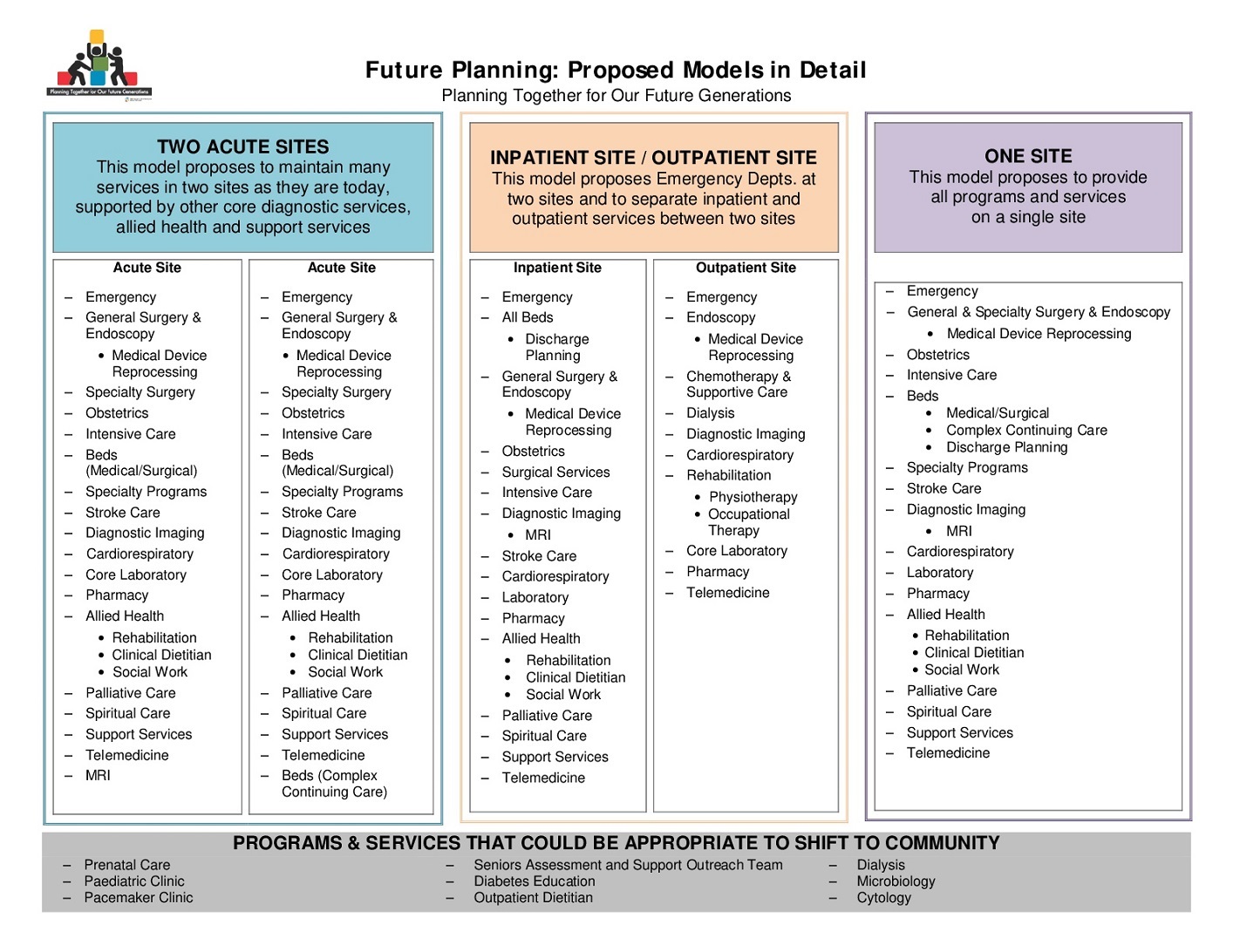
Two Acute Sites: the Two Acute Sites model proposes to maintain acute care beds and Emergency Depts., general surgery, obstetrics and intensive care at two sites. These would be supported by other core diagnostic services and allied health and support services at both sites. Specialty surgeries and programs like Chemotherapy and Complex Continuing Care that are currently single sited are proposed to continue to be in one site only. The future model also proposes to add a Stroke Rehabilitation Unit and MRI capabilities at one site.
Inpatient Site/Outpatient Site: the Inpatient/Outpatient model proposes to include Emergency Depts. at two sites and to separate outpatient and inpatient services between the sites. The Outpatient site would include services that do not require an overnight stay in hospital like endoscopies, x-rays and other diagnostic imaging, and services like chemotherapy and dialysis. The Inpatient site would include all hospital beds, surgical services, obstetrics, and intensive care, and would be supported by other core diagnostic services and allied health and support services in both sites. The Inpatient site also proposes the addition of a Stroke Rehabilitation Unit and MRI capabilities.
Detailed descriptions of the three different models are posted on the MAHC website. [Also see the image included below.]
The task force also received a land-use planning study and is awaiting the completion of an economic impact
analysis. The next task force meeting is April 9, 2018.
The Capital Plan Development Task Force members are: Cameron Renwick (Chair), Don Mitchell (Vice Chair), Scott Aitchison, Dr. Sheena Branigan, Natalie Bubela, Charlane Cluett, Dr. Caroline Correia, Dr. Keith Cross, John Curran, Jan Davidson, Peter Deane, Donna Denny, Michael Duben, Harold Featherston, Dr. Graeme Gair, Dr. Biagio Iannantuono, Dr. Jennifer Macmillan, Dr. David Mathies, Philip Matthews, Cathy McMurray, Graydon Smith, Tim Smith, Eric Spinks, Cathy Still, and Beth Ward.
Media release, April 13, 2018—Task Force Finalizes Services Proposed in Future Models
Muskoka Algonquin Healthcare’s (MAHC) Capital Plan Development Task Force has reached an important point in its future planning work, coming to consensus on the details of the programs and services proposed in each of the models.
Through many workshops with clinicians and various other stakeholders, the models have evolved from high-level concepts to more in-depth descriptions of the programs and services that are proposed in each of the models, explains Cameron Renwick, Chair of the Capital Plan Development Task Force.
“No decisions on a preferred model have been made,” says Renwick. “Throughout the process, we have received significant input that has informed the models. Many people have been involved in finalizing the programs and services proposed in each model, including MAHC leaders, staff and physicians, community providers, and municipalities. I want to assure everyone the task force is listening, and recognizes that community engagement has an important role in the evaluation of the models. I also want to remind everyone this is high-level planning for 10 to 15 years or more.”
Descriptions of the finalized proposed models are published in the Planning for the Future section of the MAHC website, including a Models on a Page document describing the programs and services proposed in each of three models at a glance and in greater detail.
“The Ministry also directed that our planning work explore and demonstrate the potential shift of appropriate services from hospital to community,” adds Renwick. “To meet that expectation, the task force has identified services that are currently provided in the hospital that could potentially be community-based in the future. This would only be possible if the greater health care system integration supported this transition.”
The task force has also approved the evaluation criteria that community feedback also helped shape, says Renwick. The task force will apply a variety of data such as projections, health care studies, and reports on land-use planning, economic impact, and costs to build and operate as part of their evaluation of the three models.
Once the task force determines it has collected all of the required information, members will complete an evaluation of the three different models to assist them in arriving at a preferred service delivery model to recommend to the MAHC Board of Directors.
Don’t miss out on Doppler! Sign up for our free newsletter here.
This states that it is an “Update” not the final report. I’m assuming that more detailed information (such as you suggested) will be forthcoming with their recommendation.
While it appears we have finally got the two acute sites model on the table and the one site off, the second model with the two different sites for inpatient and outpatient delivery is still a pretense of eventually having all the important things at one hospital which will eventually mean that whatever town gets the inpatient version will be the town that keeps it’s hospital.
I support Mayor Scotty’s call to shut down MAHC Board and this committee and start over. I think this is still an underhanded way to eventually end up with one Hospital, which is totally contrary to what the citizens in Muskoka/Parry Sound have loudly demanded.
I hope that Huntsville doesn’t become an outpatient site. Just look at Burk’s Falls to see what happens in the future to the emergency department. It gets closed!
I encourage all interested in the future of Huntsville site to push for inpatient services, beds, surgeries and stoke rehab.
This represents the first good news I received on this issue for a very long time. the cynic in me is concerned that this is simply a smokescreen to address the public outcry but the Ministry is still on their ill conceived mission.
Great chart … but where is the cost ($$) side to achieve each model proposal? Where is the future vision for each model? Where are the pros and cons for each model? Where are the service scenarios for each model? Let’s be honest .. to post this chart in the paper without impact / consequence to the area for each model is not going to solve or move this debate forward. It is just making ‘some’ of the public happy. Time for the rubber to hit the road with facts and figure($$) information for each model .. and ..short term … long term consequences / impact to the area.
I’m so happy to see the Two Acute Sites model on the table. This is exactly what most of us in Huntsville, Bracebridge and the Almaguin Highlands want and what we feel we need.
Our hope now is that the task force will recommend this model to MAHC, and that MAHC will in turn recommend it to the Ministry of Health and Long-Term Care, But I’m grateful for this first step in the right direction.
Thank you to everyone on the task force.