
A ray of hope emerged with MAHC’s recent announcement that the “not status quo” qualification was dropped, putting the community’s preferred two full acute-care site option on the table for evaluation, coming three years late. Now, a pressing concern is what costing criteria will be used in model selection? Will it be based on the 2014/15 cost data, as recently published by the MAHC board chair blog?

This cost data comparing three future hospital models is dated, and the assumptions behind the two full-service acute-care model drove the costs up.
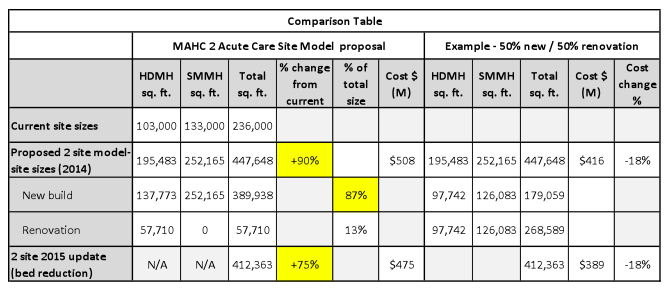
Based on the detailed numbers in the Master Plan appendices (per MAHC web site), 100 per cent of the Bracebridge site and 70 per cent of the Huntsville site were costed as new builds. This translates to 87 per cent new build, and the remaining 13 per cent full renovations.
Per the Comparison Table below, the two-site model total square footage would be 90 per cent larger (75 per cent after bed reduction) than the current two hospital sites combined. (Note: it’s also approximately 36 per cent larger than the one-site model.) It is hard to fathom what is driving this magnitude of hospital size increase.
To our knowledge, there are no hard Ministry-specified timelines associated with reaching the latest new standards for existing hospitals. If there were (within capital planning timelines of five,10 and 20 years), it would far exceed provincial affordability. (Our rough estimate: $70B+.) With our hospitals’ ages sitting at the provincial average of about 45 years, it is hard to imagine a capital plan with this much new build being approved. Lowering the level of the capital-intensive ‘new build’ would help. This would also allow staged upgrades to newer standards and facility improvements sooner.
For example, lowering to 50 per cent new build and 50 per cent renovations drops cost by close to 20 per cent:
Why does MAHC’s two-site plan have such a high space increase and ‘new build’? It certainly makes it less attractive from a cost perspective, so it must have influenced the one site recommended in 2015. There should have been a lower cost option considered.
Within the narrative of the Chair’s blog, we find other concerning comments:
- MAHC’s case in a presentation to the District of Muskoka Corporate & Emergency Services Committee (January 19) for a capital reserve ranging from $84M to $114M in support of MAHC redevelopment ‘local share’.
Our take: The apparent lack of more cost-effective options resulted in such a large local share, disrespecting Muskoka ratepayers by imposing on them the largest single capital commitment in the District’s history.
- Articulating a three-to-five year need for $39M for building infrastructure, equipment and technology. (Note: not future development.)
Our take: Knowing the bulk of this is for infrastructure capital begs questions: This need did not suddenly arise; has leadership managed their asset/replacements effectively, and along with other partners, sufficiently pressured the Ministry/LHIN to address this growing infrastructure deficit? Is a one-site future causing Ministry reluctance to invest in upgrades today? Why are we into year seven of capital planning, yet only in Stage 1 of 5 stages? At this pace, it really could be 15 years ‘at a minimum’ before anything gets done to fix the infrastructure deficit, let alone new development. Why is there such a lack of urgency?
- The Capital Plan Development Task Force was established by the MAHC board to recommend the best model ensuring “high-quality, safe and sustainable care for future generations…even if they are unpopular.”
Our take: This signals the one-site model remains, and based on some future “comprehensive process,” may yet be MAHC’s decision, even if unpopular. Critical requirements of high-quality, safety and sustainability can be driven effectively through more than the one-site model. It’s not only about future generations, but current generations as well.
Finally, the most recent update (#12) by the MAHC Capital Planning Task Force acknowledged the overwhelming consensus of the community for retaining two full-service acute-care sites. We encourage them to get on with it now. MAHC must stop claiming that ministry ‘direction and process’ forces them to do additional deep-dives/comprehensive analysis into other options that are clearly unacceptable to the community. (There should be more than sufficient data already collected to fulfil ministry needs.)
It is well past time for MAHC leadership to get on with delivering what the community has demanded, and with a new sense of urgency.
‘Listen To The People, MAHC!’
For more information, please visit the Community Advocates for Hospitals and Healthcare for Muskoka and Area (CAHHMA) website at cahhma.com and join us.
Authored by Dave Wilkin, (former) MAHC director, retired bank & IT executive, and CAHMA member, and Ross Maund, (former) MAHC director, career health services corporate executive, and CAHMA member.
Don’t miss out on Doppler! Sign up for our free newsletter here.
Here is what can happen with two hospitals serving a spread out community; http://psfdh.on.ca/
why is it that here in Muskoka, we cannot do something similar?
The area of coverage is about the same for both as well as the population base. The proximity to large urban centers is also similar (Kingston/Brockville vs. North Bay/Orillia/Barrie).
Sure, its all on MAHC’s website. Its in their Pre-Capital submission and in the Master Program Master Plan Appendix D. Here are the links: http://www.mahc.ca/en/about/resources/AppendixDRevisedJanuary2016.pdf
http://www.mahc.ca/en/about/resources/MAHCPre-CapitalSubmission2015October29-FINAL.pdf
To the MAHC Executive, The question I have concerning the single site hospital, have you factored in the additional costs to those individuals who were forced to drive that extra distance to a hospital? Those same individuals may or may not have gotten there in time because of that extra time it took to get medical attention! There certainly would be a cost factor involved, that shouldn’t be ignored.
I would like to know where the dollar amounts /numbers actually come from please ?